BMI Categories Explained: WHO Classification & Risk Levels
Complete reference for all 8 Body Mass Index categories per WHO Technical Report Series 854. Decode your BMI score with clinical interpretation, health risk profiles, and Asian-adjusted thresholds — backed by the Lancet 2016 mortality meta-analysis.
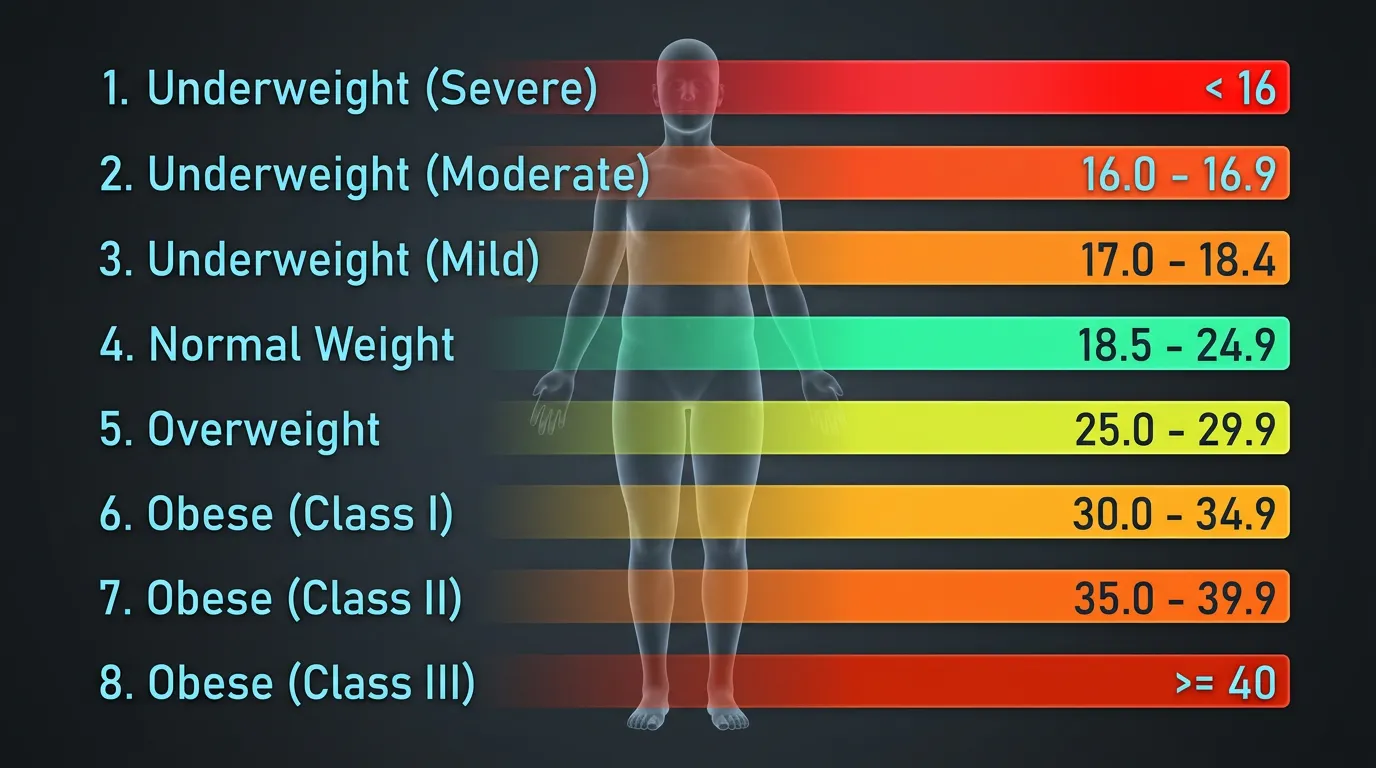
The World Health Organization classifies adult BMI into 8 clinical tiers spanning from Severe Thinness (BMI under 16) to Class III Obesity (BMI 40 or higher). Each tier corresponds to a measurable cardiometabolic risk profile validated through decades of epidemiological research. The Global BMI Mortality Collaboration (Lancet 2016, n=10.6 million) demonstrated lowest all-cause mortality at BMI 20 to 25 — narrower than the WHO "Normal Weight" range suggests.
| BMI Range (kg/m²) | WHO Classification | Risk Level |
|---|---|---|
| Below 16.0 | Severe Thinness | Very High |
| 16.0 – 16.9 | Moderate Thinness | High |
| 17.0 – 18.4 | Mild Thinness | Moderate |
| 18.5 – 24.9 | Normal Weight | Low (Optimal) |
| 25.0 – 29.9 | Overweight (Pre-Obesity) | Increased |
| 30.0 – 34.9 | Obesity Class I | High |
| 35.0 – 39.9 | Obesity Class II | Very High |
| 40.0 and above | Obesity Class III (Morbid) | Extremely High |
Source: WHO Expert Committee on Physical Status, Technical Report Series 854 (1995)
The WHO BMI Classification System
WHO Technical Report Series 854 (1995) established the 8-tier BMI classification system used globally for adult nutritional and cardiometabolic risk screening. The cutoff points were derived from large-scale mortality and morbidity data correlating BMI with all-cause death and weight-related chronic disease incidence.
The classification system organizes BMI values into three primary domains — underweight (BMI under 18.5), normal weight (18.5 to 24.9), and overweight or obese (25.0 and above). Each domain subdivides into clinically meaningful tiers based on disease risk gradients. Underweight separates into Severe, Moderate, and Mild thinness. Overweight/obesity separates into Pre-Obesity, Class I, Class II, and Class III. This 8-tier granularity supports targeted clinical intervention — from refeeding protocols for severe thinness to bariatric surgery eligibility for Class III obesity.
The cutoffs are universal in WHO documentation but require population adjustment in practice. Asian populations exhibit cardiometabolic risk at lower BMI values, prompting the WHO 2004 Expert Consultation to establish ethnic-specific overweight (≥23.0) and obesity (≥27.5) thresholds. Children and adolescents use percentile-based growth charts rather than fixed adult cutoffs. Athletes and pregnant women require alternative assessment approaches entirely.
Underweight Tiers — Severe, Moderate, Mild
BMI below 18.5 indicates underweight status across 3 severity tiers, with mortality risk rising sharply below 16.0. Underweight categories carry elevated risk for immunosuppression, hormonal dysfunction, osteoporosis, and acute mortality from electrolyte imbalance or cardiac arrhythmia.

BMI <16Severe Thinness
Severe Thinness (BMI under 16.0) represents the most critical underweight tier, correlating with approximately 2.5-fold elevated all-cause mortality compared to normal weight. Clinical risks include severe immunodeficiency, electrolyte imbalance, cardiac arrhythmia susceptibility, refeeding syndrome upon nutritional restoration, and acute organ failure. This tier requires immediate medical intervention — typically inpatient nutritional rehabilitation with cardiac monitoring during refeeding.
Severe Thinness often indicates underlying pathology: anorexia nervosa, advanced cachexia from malignancy, untreated hyperthyroidism, severe gastrointestinal malabsorption, or chronic infectious disease. Sustained BMI below 16 in adults without rapid weight gain warrants comprehensive endocrine, gastroenterological, and psychiatric evaluation.
BMI 16-16.9Moderate Thinness
Moderate Thinness (BMI 16.0 to 16.9) carries elevated risk for hormonal dysfunction including amenorrhea in women, suppressed testosterone in men, and impaired bone mineral density accrual. Cardiac function may show bradycardia, hypotension, and reduced exercise tolerance. Cognitive performance declines with chronic energy deficit, manifesting as concentration difficulty and reduced working memory.
This tier commonly affects individuals with restrictive eating patterns, endurance athletes with energy availability deficits, and patients with chronic illness. Clinical management focuses on identifying and treating underlying causes alongside structured caloric rehabilitation under medical supervision.
BMI 17-18.4Mild Thinness
Mild Thinness (BMI 17.0 to 18.4) represents the least severe underweight tier but still elevates clinical risk above normal weight. Common manifestations include reduced energy levels, increased susceptibility to infections, brittle hair and nails, irregular menstruation, and reduced cold tolerance. Long-term consequences include accelerated bone density loss and elevated osteoporosis risk in later life.
This tier frequently appears in chronically active individuals with insufficient caloric intake, those with constitutional thinness (genetic predisposition), or those recovering from acute illness. Intervention focuses on gradual caloric increase, protein optimization (1.2 to 1.6 g/kg body weight daily), and resistance training to restore lean mass.
Normal Weight — The Optimal Range
BMI 18.5 to 24.9 defines the WHO Normal Weight range, with lowest all-cause mortality occurring at the narrower band of 20 to 25 per the Global BMI Mortality Collaboration meta-analysis. This tier represents the optimal cardiometabolic risk profile for most adults outside specific populations.
BMI 18.5-24.9Normal Weight
The Normal Weight tier spans 6.4 BMI units, the widest single category in the WHO classification. This broad range encompasses substantial body composition variation — from lean recreationally active adults at BMI 19 to muscular individuals approaching 25. Within this tier, cardiometabolic risk remains lowest, although mortality data reveals important nuance about the optimum point.

The Lancet 2016 Optimal Range
The Global BMI Mortality Collaboration published the largest pooled analysis of BMI-mortality relationships in The Lancet (2016), encompassing 239 prospective studies and 10.6 million participants. The meta-analysis identified a distinct J-shaped curve with lowest all-cause mortality concentrated between BMI 20 and 25 — a narrower window than the full WHO Normal Weight range.
Lancet 2016 Mortality Optimum Data
Why BMI 18.5 to 20 Carries Elevated Risk
Despite falling within "Normal Weight," BMI 18.5 to 20 demonstrates elevated mortality risk comparable to BMI 25 to 27. The mechanism likely involves reduced metabolic reserve during acute illness, lower bone mineral density, and frequently insufficient lean mass. For older adults particularly, BMI at the lower end of the Normal range carries mortality penalties exceeding those at the moderate Overweight tier.
Asian-Adjusted Normal Range (18.5 to 22.9)
For Asian populations, the upper boundary of Normal Weight shifts downward to 22.9, reflecting elevated cardiometabolic risk at lower BMI values. South Asian, East Asian, and Southeast Asian adults exhibit insulin resistance, hypertension, and type 2 diabetes onset at BMI values where Western populations remain metabolically healthy. The Asian-adjusted Normal range of 18.5 to 22.9 better matches population-specific disease risk gradients.
Overweight (Pre-Obesity) — BMI 25.0 to 29.9
WHO designates BMI 25.0 to 29.9 as "Overweight" or "Pre-Obesity," where cardiometabolic risk begins rising 30 to 50 percent above baseline normal weight. This tier serves as the warning threshold for clinical lifestyle intervention before progression to Obesity Class I.
BMI 25-29.9Overweight (Pre-Obesity)
The WHO official terminology "Pre-Obesity" emphasizes this tier's role as a clinical warning zone. Individuals at BMI 25 to 29.9 face approximately 30 to 50 percent elevated risk for type 2 diabetes, hypertension, cardiovascular disease, and certain cancers compared to BMI 22 to 24. The risk gradient is non-linear within this range — BMI 29 carries substantially higher cardiometabolic risk than BMI 26.

WHO Standard Threshold (≥25)
The Western threshold of BMI 25 originated from mortality data in European and North American populations. Above this cutoff, multiple chronic disease risk curves bend upward at accelerating rates. The exact threshold is somewhat arbitrary — risk increases gradually from BMI 23 upward — but BMI 25 represents the inflection point where clinical screening typically begins.
Asian-Adjusted Threshold (≥23)
Asian populations exhibit cardiometabolic risk at BMI values where Western populations remain metabolically healthy. The WHO 2004 Expert Consultation established overweight as BMI ≥23.0 for Asian individuals, reflecting elevated visceral-to-subcutaneous fat ratios and earlier insulin resistance onset. A Vietnamese adult with BMI 24 should be screened for prediabetes, hypertension, and dyslipidemia — equivalent risk to a Western adult at BMI 26.
Health Implications at This Tier
Common metabolic findings include modestly elevated fasting glucose (5.6 to 6.9 mmol/L), borderline hypertension (130-139/85-89 mmHg), atherogenic dyslipidemia with triglycerides above 1.7 mmol/L, and elevated waist circumference. Many individuals at this BMI carry early-stage metabolic syndrome without symptomatic presentation. Annual lipid panels, HbA1c, and blood pressure monitoring become clinically warranted.
When to Intervene
Lifestyle intervention at this tier produces high return on effort. Modest weight loss of 5 to 10 percent of body weight significantly improves insulin sensitivity, blood pressure, and lipid profiles. Mediterranean dietary patterns, structured aerobic exercise (150 minutes weekly), and resistance training (2-3 sessions weekly) represent evidence-based first-line approaches. Pharmacological intervention is generally reserved for BMI ≥27 with comorbidities or BMI ≥30 standalone.
Obesity Class I — BMI 30.0 to 34.9
BMI 30 to 34.9 marks Class I Obesity, the threshold where GLP-1 receptor agonists become FDA-approved standalone treatment and clinical intervention becomes urgent. This tier represents approximately 2 to 3 times the mortality and morbidity risk of optimal BMI.
BMI 30-34.9Obesity Class I
Class I Obesity affects approximately 25 percent of adults in the United States and growing proportions globally. At this tier, type 2 diabetes risk increases 5 to 10-fold compared to normal weight. Cardiovascular events rise correspondingly. Quality of life metrics show measurable decline. Sleep apnea, gastroesophageal reflux disease, and osteoarthritis become substantially more prevalent.
Cardiometabolic Risk Profile
Class I Obesity typically presents with established metabolic syndrome features: fasting glucose ≥5.6 mmol/L, blood pressure ≥130/85 mmHg, triglycerides ≥1.7 mmol/L, HDL cholesterol below 1.04 mmol/L in men or 1.30 mmol/L in women, and waist circumference exceeding ethnic-specific thresholds. Three or more of these features confirms metabolic syndrome diagnosis.
GLP-1 Eligibility (Semaglutide, Tirzepatide)
FDA-approved GLP-1 receptor agonists for weight management — semaglutide (Wegovy) and tirzepatide (Zepbound) — require BMI ≥30 for standalone prescription, or BMI ≥27 with weight-related comorbidities. Class I Obesity therefore represents the modern pharmacological intervention threshold. Clinical trials demonstrate 15 to 22 percent average weight loss with these medications over 68 weeks, substantially exceeding lifestyle intervention alone.
Treatment Options
Comprehensive treatment combines pharmacotherapy with intensive lifestyle modification. Structured behavioral programs (15+ sessions over 6 months), Mediterranean or low-carbohydrate dietary approaches, supervised exercise progression, and pharmacotherapy where indicated form the standard of care. Bariatric surgery may be considered in Class I Obesity only with severe comorbidities, though guidelines generally reserve surgical intervention for Class II and III.
Obesity Class II — BMI 35.0 to 39.9
BMI 35 to 39.9 represents Class II Obesity, where bariatric surgery becomes eligible with at least one obesity-related comorbidity. Mortality risk at this tier approaches 3 to 4 times that of optimal BMI.
BMI 35-39.9Obesity Class II
Class II Obesity represents a clinical urgency tier where conservative treatment alone frequently proves insufficient. Sustained weight loss of 15 to 25 percent through lifestyle changes is rarely achievable for individuals at this BMI without pharmacological or surgical assistance. Daily functional impairment becomes common — difficulty with prolonged standing, climbing stairs, and physically demanding tasks.
Bariatric Surgery Eligibility (with Comorbidity)
The American Society for Metabolic and Bariatric Surgery (ASMBS) guidelines establish BMI 35 to 39.9 with at least one obesity-related comorbidity as standard bariatric surgery indication. Qualifying comorbidities include type 2 diabetes, severe sleep apnea (AHI ≥30), uncontrolled hypertension requiring multiple medications, non-alcoholic steatohepatitis, debilitating arthritis, or severe gastroesophageal reflux disease. Sleeve gastrectomy and Roux-en-Y gastric bypass represent the most common procedures.
Clinical Risk Stratification
Comprehensive evaluation at this tier requires cardiac risk assessment (often including stress testing), pulmonary function evaluation, sleep study for apnea screening, hepatic function panels including liver fibrosis assessment, and comprehensive metabolic panels. Many patients carry undiagnosed conditions requiring management before any surgical intervention.
Obesity Class III (Morbid) — BMI ≥40
BMI 40 or higher defines Class III (Morbid) Obesity — the threshold for standalone bariatric surgery eligibility without requiring comorbidities. This tier reduces life expectancy by 10 to 14 years compared to optimal BMI 22 to 24.
BMI ≥40Obesity Class III (Morbid)
Morbid Obesity carries the highest cardiometabolic risk profile in adult BMI classification. Type 2 diabetes prevalence approaches 50 percent at this tier. Cardiovascular events occur at 4 to 5-fold elevated rates compared to normal weight. Surgical intervention becomes the most effective long-term treatment, with bariatric procedures producing sustained 25 to 35 percent total body weight loss over 5+ years.

Standalone Bariatric Eligibility
ASMBS guidelines establish BMI ≥40 as standalone bariatric surgery indication without requiring comorbidities. The risk-benefit calculation overwhelmingly favors surgical intervention at this tier — perioperative mortality below 0.3 percent versus 10-14 year life expectancy reduction without treatment. Sleeve gastrectomy, Roux-en-Y gastric bypass, and biliopancreatic diversion with duodenal switch represent the primary procedural options, each with distinct weight loss, comorbidity resolution, and complication profiles.
Life Expectancy Impact
Class III Obesity reduces life expectancy by approximately 10 to 14 years compared to BMI 22 to 24. Cardiovascular disease accounts for approximately 60 percent of the excess mortality. Cancer-related deaths (particularly esophageal, colorectal, renal, pancreatic, breast post-menopausal, and endometrial) account for an additional 20 percent. Diabetes-related complications, sleep apnea sequelae, and kidney disease contribute the remainder.
Treatment Urgency
Conservative treatment alone rarely produces sustained meaningful weight loss at this BMI. Multidisciplinary care becomes essential — bariatric medicine specialists, registered dietitians, mental health providers, exercise physiologists, and surgical teams. The 2023 AMA Policy H-440.842 emphasizes that BMI 40+ patients warrant immediate comprehensive evaluation rather than prolonged lifestyle-only trials.
Asian-Adjusted Categories — A Critical Note
Asian populations require adjusted BMI thresholds: overweight ≥23.0 and obesity ≥27.5 per WHO 2004 Expert Consultation. These adjustments reflect elevated cardiometabolic risk at lower BMI values across South Asian, East Asian, and Southeast Asian populations.
| Classification | WHO Standard | WHO Asian-Adjusted |
|---|---|---|
| Normal Weight | 18.5 – 24.9 | 18.5 – 22.9 |
| Overweight | ≥ 25.0 | ≥ 23.0 |
| Obese | ≥ 30.0 | ≥ 27.5 |
Source: WHO Expert Consultation on Appropriate BMI for Asian Populations (Lancet, 2004)
The biological basis for these adjustments includes higher visceral-to-subcutaneous fat ratios at equivalent BMI, earlier insulin resistance onset, greater type 2 diabetes susceptibility, and elevated cardiovascular risk gradients. Indian, Chinese, Japanese, Korean, Vietnamese, Thai, and Filipino adults exhibit metabolic syndrome at BMI values where Western populations remain healthy.
What These Categories Don't Tell You
BMI categories cannot account for body composition, ethnicity, age, muscle mass, or fat distribution. Athletes register as "obese" despite low body fat; sarcopenic seniors appear "normal" despite dangerous visceral adiposity; metabolically obese normal-weight individuals escape detection entirely.
The classification system provides population-level screening utility but requires contextual interpretation for individuals. The AMA 2023 Policy H-440.842 formally acknowledged these limitations and recommended BMI be used alongside waist circumference, body composition analysis, and metabolic markers — not as standalone diagnostic.
Frequently Asked Questions
A normal BMI for adults is between 18.5 and 24.9 kg/m² per WHO classification. However, the Global BMI Mortality Collaboration meta-analysis (Lancet 2016) identified BMI 20 to 25 as the narrower optimal mortality range. Asian populations should use adjusted thresholds: normal range 18.5 to 22.9.
The WHO classifies adult BMI into 8 clinical tiers: Severe Thinness (BMI under 16), Moderate Thinness (16.0-16.9), Mild Thinness (17.0-18.4), Normal Weight (18.5-24.9), Overweight or Pre-Obesity (25.0-29.9), Obesity Class I (30.0-34.9), Obesity Class II (35.0-39.9), and Obesity Class III or Morbid Obesity (≥40).
Morbid obesity is defined as BMI 40 or higher, classified as Obesity Class III by WHO standards. This threshold qualifies individuals for standalone bariatric surgery eligibility without requiring comorbidities. Class III Obesity is associated with 10 to 14 years of reduced life expectancy compared to optimal BMI 22 to 24.
Yes, WHO BMI classification ranges are identical for adult men and women. However, body composition at equivalent BMI differs significantly: women typically carry 8 to 10 percent more body fat than men at the same BMI value due to hormonal and reproductive physiology. Sex-specific body fat percentage assessment provides more accurate composition data.
Bariatric surgery eligibility requires BMI 40 or higher standalone, or BMI 35 to 39.9 with at least one obesity-related comorbidity such as type 2 diabetes, severe sleep apnea, cardiovascular disease, or non-alcoholic fatty liver disease. These thresholds are established by the American Society for Metabolic and Bariatric Surgery (ASMBS).
Pre-obesity is the WHO official term for BMI 25.0 to 29.9, commonly called Overweight. This tier indicates increased cardiometabolic risk approximately 30 to 50 percent above baseline normal weight. Pre-obesity serves as the clinical warning threshold where lifestyle intervention is most effective before progression to Class I Obesity (BMI 30+).

Find Your BMI Category Instantly
The VisualBody Clinical BMI Calculator displays your exact tier classification with Asian-adjusted thresholds, target healthy weight range, and full risk interpretation — all in seconds.
Open BMI CalculatorBased on Scientific Sources
- WHO Expert Committee on Physical Status. Physical Status: The Use and Interpretation of Anthropometry. WHO Technical Report Series 854; 1995. → PubMed
- Global BMI Mortality Collaboration. Body-mass index and all-cause mortality: individual-participant-data meta-analysis of 239 prospective studies. The Lancet; 2016. → PubMed
- WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. The Lancet; 2004. → PubMed
- American Society for Metabolic and Bariatric Surgery. Eligibility for Metabolic and Bariatric Surgery; 2022. → ASMBS Guidelines